By Anna Reser
In 2007, a controversy erupted over a paper in a pediatric medical journal about a set of therapeutic surgeries and drug treatments designed to attenuate the growth and development of six year old Ashley who had been diagnosed with static encephalopathy. Ashley’s parents argued that the treatment would improve Ashley's quality of life by making it easier for them to care for her, and by relieving the discomfort of a functioning female reproductive system. Ashley’s uterus and breast buds were removed, and she was given drug treatments to stunt her growth. The case, known as “The Ashley Treatment,” has been used by biomedical ethicists to explore many of the issues related to reproductive health and freedom for women with disabilities, and to examine the ethics of how caregivers “manage” the bodies of disabled women whom they care for.
The main criticism leveled at Ashley’s parents was that they authorized drastic medical interventions simply for their own convenience. By arresting Ashley’s growth and removing her reproductive organs, they would be saving themselves a great deal of physical labor. Ashley’s parents, and the physician who performed the treatment, argued that this type of therapy would prevent Ashley from becoming institutionalized and allow her parents to care for her at home. As for the surgical interventions, Ashley’s parents cited the prevention of pain and the preservation of her “dignity.” The removal of Ashley’s breast buds would prevent the development of her breasts, and as her parent’s argued, eliminate the risk of breast cancer later in life. A hysterectomy would prevent both menstruation and pregnancy. By removing Ashley’s reproductive organs and suppressing the development of her secondary sex characteristics, the caregivers and doctors argue that her body would more closely match her cognitive state which would remain at the level of an infant for her entire life.
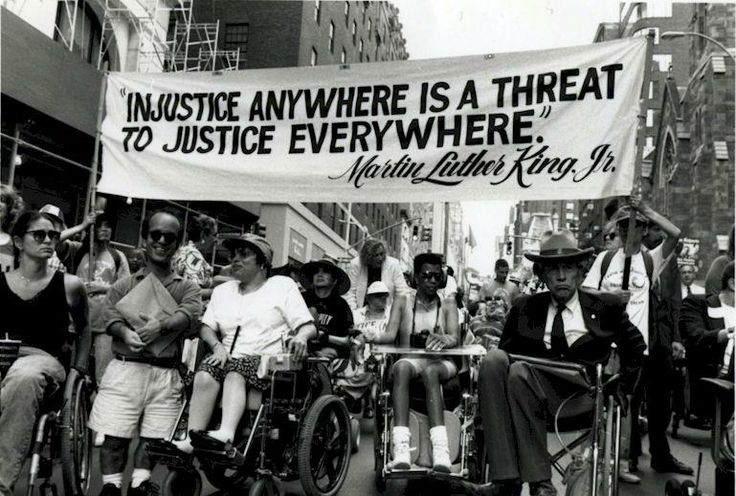
Disability activists and scholars developed a new framework for understanding disability as a social system of oppression that operates independently from the actual bodies of individuals.
Biomedical ethicists have argued that Ashley’s parents can only be considered to have acted ethically and in Ashley’s interest if the measures they took to alter Ashley’s body were necessary out of a lack of other options and social support. This case goes to the heart of the problems that disability activists and scholars describe as the medical model of disability, which sees impairment and disability as interchangeable. This model casts disability as a factual, physical state of being that is attached to an individual body. It relies on highly articulated modern systems of medicine that focus on the individual pathologization of bodies against an idealized “normal body.” This is the fulcrum of modern medicine’s diagnostic power. But it has also historically prevented people with disabilities from claiming a coherent political identity; when the medical establishment insists on the individual physicality of disability, it is difficult to form solidarity with people with different types of disabilities.
This model necessarily results in the kind of segregated accommodations that mirror medicine’s central normal/pathological distinctions—not to mention racial segregation. In response, disability activists and scholars developed a new framework for understanding disability as a social system of oppression that operates independently from the actual bodies of individuals. In this model, disability is the social exclusion that is imposed on people with impairments. It says that most, if not all limitations, caused by impairment can be removed, not by medical interventions on individual bodies, but by altering the social structure in which people with impairments live in order to accommodate them.
I think Ashley’s case is actually a difficult one to process through a social model of disability, something that her parent’s have attempted to argue. But her case does illustrate some ways in which a medical model of disability, combined with a historical tendency for modern medicine to pathologize the female reproductive body, creates a dangerous situation for women and girls with disabilities.
A briefing paper from 2002 by the Center for Reproductive Rights outlines a human rights framework for ensuring that women with disabilities are treated equally and ethically with regard to reproductive health. The paper outlines four areas in which measures must be taken to protect women with disabilities: 1) the right to equality and nondiscrimination; (2) the right to marry and found a family; (3) the right to reproductive health, including family planning and maternal health services, information, and education; and (4) the right to physical integrity. The last right of physical integrity encompasses the most serious consequences of the violation of the other four rights. Forced sterilization, forced abortion, the removal of reproductive organs without consent, all have been deployed as ways to control what is seen as the pathological sexuality of disabled women.
[Ashley's] case does illustrate some ways in which a medical model of disability, combined with a historical tendency for modern medicine to pathologize the female reproductive body, creates a dangerous situation for women and girls with disabilities
In Ashley’s case, we can look closely at the language that her physicians and parents use to describe her condition, and the way they perceive the harm they believe they are protecting Ashley from. Coded into this language are assumptions about “normal” bodies, which are derived from the pervasive influence of a modern medical establishment that attaches disability to individual bodies and pathologizes the female body. Ashley’s father insists that the treatment would help to preserve Ashley’s dignity, but this implies that bodily functions like menstruation are by default undignified. He further describes menstrual cramps as “chronic pain,” from which the treatment would protect Ashley. Given the documented difficulty that women face in having their chronic pain diagnosed, the language here stings. More troubling, Ashley’s parents’ concern about pregnancy, which could only occur through assault, calls up the despicable rape-culture idea that women are to blame for their reproductive capacity in the event that they become pregnant through rape.
The struggle to create equal social environments for people with disabilities is impossible to separate from other issues of identity and equality. Many people with disabilities experience intersecting oppressions based on race, gender, or class. One of the more significant failings of the 20th century disability rights movements was its lack of integration with other identity movements, particularly feminism. Beyond the specific details of individual cases, Ashley’s case illustrates that the very language we use to describe and justify medical and ethical decision making comes from and reinforces a culture of medicalization. Key to creating such intersectional identity movements is understanding the ways that professionalized science and medicine have contributed to the pathologization of women’s bodies, especially those that function outside what medicine considers the norm—an able-bodied white male body.
A key part of making the social model a reality for people with disabilities is challenging the medical establishment in a fundamental way. Critical science studies has challenged the scientific establishment’s claim on the truth, and in the process showed how bias and even racism and other oppressive ideologies have infiltrated and even shaped scientific inquiry. Medicine must be subjected to the same scrutiny. By interrogating the accepted image of the “healthy” “normal” body, we can see how modern medicine has constructed this body, not in opposition to some “objectively” pathological bodies, but in opposition to socially and culturally unacceptable bodies.
Further Reading
Matthew Liao, Julian Savulescu and Mark Sheehan, “The Ashley Treatment: Best Interests, Convenience, and Parental Decision-Making,” Hastings Center Report vol. 37, no. 2 (2007): 16-20.
Lady Science is an independent magazine that focuses on the history of women and gender in science, technology, and medicine and provides an accessible and inclusive platform for writing about women on the web. For more articles, information on pitching, and to subscribe to our newsletter, visit ladyscience.com.