
This piece has been adapted from Covid Year Three, an episode of Death Panel released earlier this month. It presents an incomplete timeline of the sociological production of the end of the pandemic across 2022. What follows is the second part of a three-part series; Part I is available here.
+
FEBRUARY 2022
February is the month that the final remains of state mask mandates went away.
In early February, a group of states announced the end of many of the last remaining mask mandates both statewide and in schools. By the end of February, the CDC introduced its “Community Level” system for its masking guidance, newly prioritizing hospitalization figures over new cases and covid transmission for determining guidelines.
Many who organize or advocate around covid will remember this moment clearly as a de facto CDC endorsement of the end of universal masking.
It’s important to note that masking was already gone in most of the country. Only eight states still had statewide mask mandates in place, along with a small number still mandating masking in schools. By this point, some states had outright banned mask mandates. In ten states, mask mandates had never been implemented at the state level in the first place, and still have yet to be at any point during the pandemic. There was still a federal transportation mask mandate in place for things like planes and public transport, though this would ultimately be struck down by a judge in April.
Additionally, as we document in an episode of Death Panel released this week, “How Liberals Killed Masking,” the key moment in undoing mask mandates and universal masking actually came when the CDC changed its masking guidance on May 13th 2021, emphasizing that vaccinated people no longer needed to mask indoors or outdoors.
At that time (spring of 2021), mask mandates were still in place in roughly half of states. At least seventeen states were due to see their mask mandates expire in the following weeks, meaning that they would have to decide whether to renew them or simply let them expire. Following the CDC’s surprise announcement, those seventeen states allowed their mask mandates to expire. Although the CDC would reverse its guideline change in July, the damage was done—those seventeen states never reinstated statewide mask mandates.
+
At the beginning of February 2022, with cases still enormously high and some 18,000 people dead from covid in the first week of February alone, states started either peeling back mask mandates, or announcing that they would shortly do so, starting with New Jersey, California, and New York, followed shortly by Rhode Island, Massachusetts, and Illinois.
All of these states announced they would drop their mask mandates around the same time. The reason this was more or less coordinated is made clear in contemporaneous reporting. On February 8th, the New York Times characterized the events as follows:
The easing of New York’s pandemic restrictions on businesses comes as Democratic-led states from New Jersey to California have announced similar moves this week, in a loosely coordinated effort that is the result of months of public-health planning, back-channel discussions and political focus groups that began in the weeks after the November election.
It was Gov. Philip D. Murphy of New Jersey who began the effort last fall, weeks after he was stunned by the energy of right-wing voters in his blue state, who nearly ousted him from office in what was widely expected to be an easy re-election campaign. Arranging a series of focus groups across the state to see what they had missed, Mr. Murphy’s advisers were struck by the findings: Across the board, voters shared frustrations over public health measures, a sense of pessimism about the future and a deep desire to return to some sense of normalcy.
Then, Omicron hit, delaying any easing of restrictions.
But slowly, as case rates began to fall again in January, conversations between Mr. Murphy’s aides and senior officials in other states began to pick back up. No actions could be taken until the virus eased its grip, the officials acknowledged.
Last week, they took their concerns to the White House. As members of the National Governors Association gathered for a meeting in the East Room, several asked President Biden to provide clear guidelines for their states to move from the crisis footing of a pandemic to a recognition that the virus was here to stay—and that it could be managed without completely upending daily life.
Other events similarly demonstrate that by November 2021, elected Democrats and liberals in the media were increasingly adopting a view that moving right on covid protections should be a part of the their 2022 electoral strategy. On November 15th, conservative Democratic party-aligned think tank Third Way published a memo following Terry McAuliffe’s prominent loss in an election for Governor of Virginia. The memo argued that “School closures + COVID policy were a bigger factor than CRT.”
This memo quickly went around in liberal policy and media circles, and the idea that covid protections would hurt Democrats in the upcoming election soon became establishment wisdom, despite the clear ideological underpinnings of its source, Third Way. The idea was prominently featured in articles in the New York Times and elsewhere. On November 23rd, Ezra Klein tweeted “Dems can't pretend COVID policy doesn't have political consequences, and there'll be a lot of on-the-margin decisions they need to make about masking and school ordinances in the coming year.”
We raise this in part because some people look at only one thing in particular as a smoking gun on masking, which is the letter sent by Biden’s polling firm Impact Research on February 24th. Impact Research told Biden in no uncertain terms to “take the win” on covid by rolling back covid protections, explicitly in order to improve their chances in the upcoming midterm elections.
While this letter is significant evidence informing their strategy going forward, based on our timeline, it seems clear that the Biden administration’s specific changes on masking guidance and the forthcoming Community Level system were already in motion by the time Impact Research’s letter arrived. As in most hegemonic constructs, while there are certainly key turning points, the aggregate effects of many key moments of social reproduction and knowledge production can’t be discounted when trying to assess what caused a particular state action to occur.
+
On February 9th the New York Times ran the following headline:
“We Are Not There Yet’: As States Drop Mask Rules, the C.D.C. Stands Firm”
From that story:
The White House has been meeting with outside health experts to plan a pandemic exit strategy and a transition to a “new normal,” but the behind-the-scenes effort is crashing into a very public reality: A string of blue-state governors have gotten ahead of President Biden by suddenly abandoning their mask mandates.
Public health experts agree that school mask mandates should not last forever, but are divided about whether it is time to drop them. The C.D.C.’s current masking recommendations advise state and local officials to enact indoor masking policies in areas of the country where transmission is high.
A color-coded map on the agency’s website shows the entire country in red; 99 percent of all counties are in a high transmission zone — a point Dr. Walensky underscored on Wednesday.
The public is understandably confused.
…
The meetings with outside experts appear to have been prompted by a trio of articles published in January in the Journal of the American Medical Association, in which six former Biden transition advisers urged the administration to take a longer view and begin drafting a pandemic playbook aimed at “the new normal.”
The effort was led by Dr. Ezekiel Emanuel, an oncologist and medical ethicist who advised former President Barack Obama. In the first article, Dr. Emanuel, Dr. Gounder and Dr. Osterholm, an epidemiologist at the University of Minnesota, wrote that the United States must avoid becoming stuck in “a perpetual state of emergency.”
To be better prepared for inevitable outbreaks—including from new coronavirus variants—they suggested that the administration lay out goals and specific benchmarks, including what number of hospitalizations and deaths from respiratory viruses, including influenza and Covid-19, should prompt emergency mitigation and other measures.
As we observed in Part I, a major theme of early 2022 was the advancement of the idea that case counts no longer mattered, and that the metrics we should now be considering are hospitalizations and deaths. While we can be certain that the advisors listed above were not the only people suggesting this to the Biden White House (Ashish Jha was also promoting this idea at the same time) the Biden administration was searching for some rationale like this.
After all, some days later, on February 21st, just four days before unveiling the CDC’s new Community Level system, Rochelle Walensky would appear on Andy Slavitt’s podcast and say the following of masking:
“I just know people are tired. The scarlet letter of this pandemic is the mask. It may be painless, it may be easy, but it’s inconvenient, it’s annoying, and it reminds us that we’re in the middle of a pandemic.”
+
On February 25th, the CDC updated its recommendation guidelines for which counties should require masking, introducing the Community Level system still in place today. The following will describe the change in brief; for a more detailed analysis we recommend our episode of Death Panel from when the change was announced, which is called “Lying Like A State.”
Previously, the CDC made masking recommendations based on covid transmission. Transmission, full stop. This was because new cases are what leads to deaths; for that matter, new cases are also what leads to new cases of long covid. It’s not particularly complicated: in order to die from covid, you have to actually catch covid first, making transmission an enduringly useful metric.
The new system changed that to deprioritize cases and transmission. The simple explanation first:
Until the CDC changed their masking guidance, their transmission map, which is the visualization of how prevalent covid spread is and where masks should be recommended, was bright red, with nearly every US county filled in at “High” transmission. This is still the case, in fact: you can still see the old map if you try—it’s just no longer used to set federal public health guidance.
Under the new guidelines, the map immediately turned a discomfiting shade of pastel green. All of a sudden, masking wasn’t recommended by the CDC in 70% of the country.
Recall that almost no states even had a mask mandate by this point. Before the CDC made this change, those states had been universally going against CDC guidance. The CDC basically changed its guidelines to say, “Yeah, sure, ok.”
Headlines in major media outlets at the time focused on this 70% figure, followed by updates in early March that masking was no longer recommended for 90% of the population. Almost no press focused on the fact that the CDC had simply changed how covid risk was calculated. The overwhelming message conveyed by this change was therefore that covid was, biologically, no longer as much of a threat as it had previously been; a far cry from the reality.
A more technical explanation of the Community Level system is this:
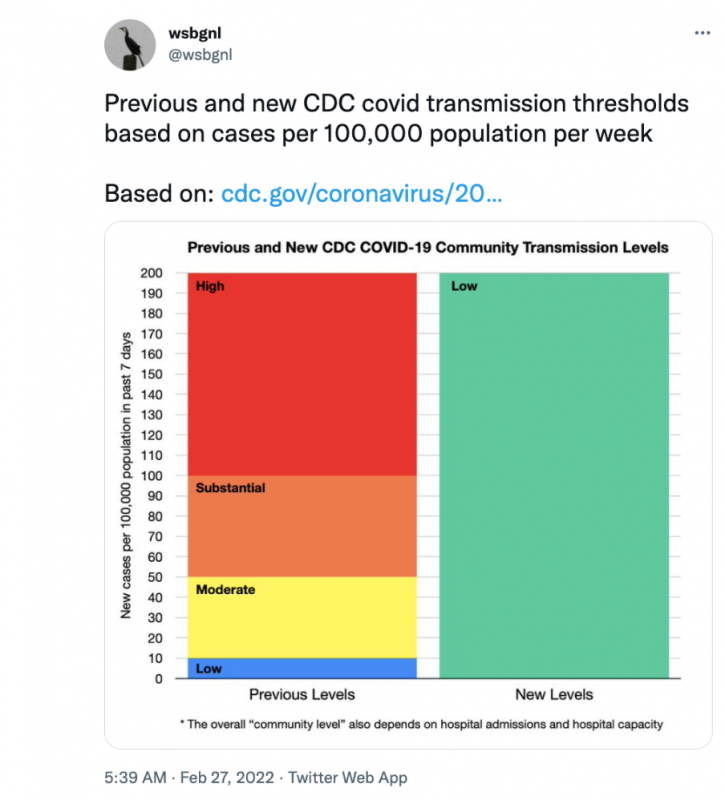
The CDC used to declare a county “High” covid risk—meaning masks should be worn there, appearing bright red on the map—if transmission was happening at a level of 100 cases per 100,000 people.
Under the new metric, covid cases themselves do not even count toward the guideline determination until there are twice that amount of cases—200 cases per 100,000 people.
In other words, under the new system you can have twice the rate of covid transmission that would previously have qualified as “High” risk level in the area where you live, and your area will still be counted as “Low.” Here is a useful visualization of this:
This new substantially higher threshold for cases is used really only as a modifier for the new principle metrics taken into account to calculate community levels. These are the following:
- New COVID-19 admissions per 100,000 population (7-day total) — in other words, at what rate new covid hospitalizations are occurring.
- Percent of staffed inpatient beds in use by COVID-19 patients (7-day average) — the percentage of occupied hospital beds, in other words, hospital capacity.
One of our favorite analogies used to explain this system comes from our colleague Nate Holdren: if you replace “covid” with “drunk driving” in this system, then while the old system was like saying, “Hey friend, you’ve had a lot to drink. Let me call you a cab,” the new system is more akin to saying, “Hey friend, you’ve had a lot to drink. Let me Google how many open hospital beds there are in the area real quick before you go ahead and drive home.”
+
It’s worth noting that the Biden administration was quite proud of this new system.
By this point, we know that they were looking for a way to communicate that people could relax on covid, while being eager to avoid a repeat of the previous year’s “declaration of independence from the virus.” So when they announced the change in metrics, it was described as a win. Walensky justified the move in the CDC telebriefing announcing it:
We wanna give people a break from things like mask wearing when our levels are low and then have the ability to reach for them again, should things get worse in the future.
This updated approach focuses on directing our prevention efforts towards protecting people at high risk for severe illness and preventing hospitals and healthcare systems from being overwhelmed. … Please remember that there are people who remain at higher risk for COVID 19 and who may need additional protection. … Those people might choose to take extra precautions regardless of what level their community is in.
+
60,351 people died of covid in the US in February.
40% of those were vaccinated. Further, 15% of the 60,000 were boosted.
MARCH 2022
The introduction of the Community Level system enabled pundits to be even more extreme in their pronouncements about masking and other covid “restrictions,” as media figures love to call them.
Here’s David Leonhardt from March 9th, 2022, in a newsletter called “Do Covid Precautions Work?” with the subheader, “Yes, but they haven’t made a big difference.” Leonhardt writes:
I’ve come to think of the point this way: Imagine that you carry around a six-sided die that determines whether you contract Covid, and you must roll it every time you enter an indoor space with other people. Without a mask, you will get Covid if you roll a one or a two. With a mask, you will get Covid only if you roll a one.
You can probably see the problem: Either way, you’ll almost certainly get Covid.
The guideline change had some other obvious effects, including a series of articles across media outlets stepping in to provide, essentially, self-help guidance for people who were still masking. Here are two examples:
March 4th, Huffington Post: “How To Cope When You’re The Only One Wearing A Mask At Work.”
March 13th, NPR: “Some people aren't ready to stop masking, but it can be tough to go against the grain.”
+
On March 1st, Biden delivers his State of the Union address, maskless, of course, to a room full of maskless people over seventy that we collectively call “Congress.”
Politico’s headline for this is: “The masks come off at Biden’s State of the Union address.”
In the speech itself, Biden touted the CDC’s community level guideline change as one of his administration’s accomplishments, saying:
Just a few days ago, the CDC issued new mask guidelines. Under these new guidelines, most Americans in most of the country can now be mask free. …
We can end the shutdown of schools and businesses. We have the tools we need.
That same day, the Biden administration released an updated version of its “National COVID-19 Preparedness Plan.” It was sold as a bold new agenda for how the White House wanted to move forward; in reality, the plan is quite miserable, an early feint toward pushing all covid treatments and care toward the private market.
The Washington Post described this announcement as such: “White House unveils plan to move America past covid crisis, says shutdowns no longer necessary.”
So what was in this plan?
It was our first introduction of Test to Treat, the program of making Paxlovid available to be prescribed at the pharmacy. As a matter of policy, this continued the administration’s broader prerogative of relying on major pharmacy chains like CVS and Walgreens to be the first line of public health administration on covid. As we’ve all seen, this strategy does not work out great.
The plan also bluntly states the following:
“We look to a future when Americans no longer fear lockdowns, shutdowns, and our kids not going to school” … “It’s a future when the country relies on the powerful layers of protection we have built and invests in the next generation of tools to stay ahead of this virus.”
Despite touting “layers of protection”—one of the most basic layers of protection, by far, is masking, which the administration had been working to undo—the plan also says this (emphasis added): “Masks have been a critical tool to protect ourselves, but they have a time and a place.”
Additional goals in the document include a pledge to “support broad access to free testing across the country.” This is, as readers who have gotten this far in the timeline will undoubtedly know, ironic considering that the Biden administration would promptly do just the opposite, dismantling testing infrastructure across the country, or allowing it to be closed without taking federal action to keep it running.
And yet, in the words of the Biden covid plan, the Biden administration has “successfully put equity at the center of a public health response for the first time in the nation’s history.”
+
March 2022 also marks the emergence of something that would define the rest of the year, which is Biden’s weak attempts to make Congress continue to fund the covid response
We won’t be exhaustive about this interminable part of the year, but in summary: by mid-February, Biden’s HHS had informally asked Congress for about $30 billion to keep funding the covid response, including the vaccines and therapeutics that the federal government is, at time of writing, still paying for. In early 2022, the federal government was still paying for covid care for uninsured people, an undoubtedly important component of a pandemic response for a country where healthcare is a privilege for those who can afford it. That program, which covered covid care for uninsured people, was unceremoniously killed March 22nd, 2022, when the Biden administration and Congress allowed its funding to run out.
Around the state of the union, the Biden administration finally got around to formally asking congress for funding. They painted the picture as extremely urgent and dire, but then, just days later, counteracted their own message by substantially reducing their funding target. This pattern would play out continually over the course of the year, allowing the Biden administration to paint Congress as the central reason the covid pandemic continues to be such a disaster, while simultaneously normalizing covid in every other way possible, diminishing the sense of political urgency.
+
Immediately after this, it appears that a conversation gets prioritized within the White House while simultaneously getting hidden from the public for most of the year: preparations to kick covid vaccines and treatments to the private market by 2023.
In Biden’s March 2022 “National COVID-19 Preparedness Plan” the Administration hinted at this transition in the following way under the header “Explore public and private insurer coverage of COVID-19 treatments this year,” in a longer list of their immediate goals (emphasis added):
The Administration has worked during the pandemic to ensure that COVID-19 treatments are free and accessible to all Americans. … Under the Administration’s current model for distributing effective treatments against COVID-19, treatments are free to the public and distributed directly to states and territories and to community health centers across the country to ensure equitable access in our hardest-hit communities. The Administration also reimburses providers for the cost of administering COVID-19 treatments to the uninsured. To ensure that these treatments remain accessible and to reduce the ongoing costs to the federal government, the Administration will work with insurers and Congress to explore public and private insurer coverage of COVID-19 treatments this year.
No timeline is given for this goal, so it goes largely ignored until August of 2022, when the administration starts making more official announcements about it. However, by June, we see the first indication of a time horizon, when Ashish Jha says unprompted in an interview with Bob Wachter that, while talking to members of Congress, he has to explain to them that covid care can enter the private market in “maybe 2023.” We cover this statement as a significant development on Death Panel, but at the time, almost no one picks it up.
That said, on March 15th 2022, the administration does telegraph this shift more substantially, though, again, no timeline is suggested. The following is from the transcript of a press call with an unnamed “Senior Administration Official” who, from word choice and manner of address, we presume to be Jeff Zients, who was at that time still the White House coronavirus response coordinator:
MUNOZ: Let’s go to Tamara Keith at NPR.
Q: I’m hoping that you can sort of explain the mechanics of the markets for these various things, like why the government still needs to be involved in making these large purchases; why, you know, large hospital groups couldn’t be buying the vaccines or buying the monoclonal antibodies; like, why—why it is all so contingent on federal funds.
SENIOR ADMINISTRATION OFFICIAL: Yeah. Tamara, it’s a good question.
Look, in our preparedness plan, we outlined that we want to explore in the future the ability to transition some of COVID treatments and potentially other tools to insurance-based market, like other healthcare. … [W]e want to explore over the long term a safe, a smooth transition. But right now, we have immediate needs, and we need Congress to act.
MUNOZ: Let’s go to Zeke Miller at the AP.
Q: Hey. Thanks for doing this. Just to follow up on Tam’s question there: So, why not, if—you know, if the need is immediate and Congress right now shows no sign of budging, aren’t you exploring those alternate avenues? You know, you just required private insurers to cover the cost of at-home tests. Why not have them cover the cost of vaccines and Paxlovid and other things like that?
Why does the government still need to be the middleman there, given the current rate of COVID-impacted society and mortality? I mean, how is that different than, you know, cancer or heart disease, other things where insurance is — the private insurance market is already effective there? …
SENIOR ADMINISTRATION OFFICIAL: Thanks, Zeke. So, on your first question, I’d say, look, we are exploring those alternatives. We made that clear in the—in the Preparedness Plan that we released a few weeks ago. But it takes time, as you know, to move to that—to such a system. We—it needs to be an orderly, smooth transition. So we’re working through that. … So it’s certainly something we’re exploring.
+
Presuming the “Senior Administration Official” in that call is Jeff Zients, this turns out to be one of the last major acts he would take while covid czar. On March 17th, Ashish Jha is officially announced as the new hire for the job.
As we said at the time, our general impression is that Jha is brought in largely to make everyone feel more positively about the Biden administration.
Progressive media outlets had lobbied plenty of criticism at Zients by the time Jha was announced to replace him. Much of that criticism, however, centered exclusively on Zients’ lack of a public health background and his (certainly damning) career in private equity. Jha fit the bill as someone who could alleviate those concerns: the Dean of a public health school—notwithstanding the largely administrative role of Deans in academia—and, most importantly, someone who had been, for better or worse, playing TV doctor to the country for the better part of the covid pandemic. STAT News had called him, in early 2021, “TV’s everyman expert on covid.” And now, in a move that certainly would have made the press aghast in the Trump era, the White House had essentially decided, “Get me the guy from TV.”
+
About 30,000 people died of covid in the US March.
43% of those, or about 12,000 people, were fully vaccinated. Further, 20% of those 30,000 deaths were in people who were also boosted.
APRIL 2022
This brings us to April. But let’s stay on breakthrough deaths for a second.
As we mentioned in Part I [link], in April, the CDC finally updates one of its datasets that had been dormant for months, tracking deaths by vaccination status in 27 jurisdictions.
On April 21st, 2022, the Kaiser Family Foundation released a report on this dataset. On Death Panel, we also covered this in an episode called “Breakthroughs.” That episode—not the episode itself, but the existence of the episode—pissed off a lot of liberals, and added fuel to an interminable discourse in early April that to be concerned about breakthrough deaths was to fall prey to “the base rate fallacy.” This argument was always nonsense—the US vaccination rate was and remains piss-poor—so we won’t revisit or re-litigate it in full here. But the important claim is this:
Until this point, the main arguments demonstrating that the “pandemic of the unvaccinated” line was both incorrect and grossly stigmatizing were rhetorical. We could reference the many anecdotal cases of breakthrough deaths, or the inconsistent handful of states that reported them. And we did that. But this was the first systematic look at how common breakthroughs are. By the end of April, even the Washington Post prominently acknowledged this with the headline “Covid deaths no longer overwhelmingly among the unvaccinated as toll on elderly grows,” although they couched this claim in a framing device the Post would call, by late November, “a plague of the elderly.”
For us, this new information was a pretty frightening validation of something we’d been saying for a long time: the vaccine-only strategy pursued by the Biden administration does not work. We still need, in 2022, layered protections—layered protections just like the masks that the Biden administration said in March that there was “a time and a place for.”
There’s one last tragic point on this.
As of April, none of us knew it yet, but April 2022 is the first month where a majority of the people dying are fully vaccinated.
And not by a small margin either. 59% of covid deaths in April were in people who were fully vaccinated.
This means that while liberals were yelling at us—and the Kaiser Family Foundation, and the Washington Post—about the Base Rate Fallacy and how we were undermining Biden’s covid response, more than half of people dying of covid were vaccinated. All just after the Biden administration had just done so much work to undo what remained of masking and other pandemic protections in the US.
+
The major policy development of April came on April 18th, when a federal judge struck down the TSA’s transportation mask mandate, one of the last major remaining mask mandates.
What did the Biden administration do in response? Did they turn immediately to say, “We will fight this”?
Nope. At first, they just … dithered. They called the ruling “disappointing” and took the opportunity to essentially stress to people that you could still make an individual decision to mask on an airplane or on the bus, if you really want to.
Before the Biden administration can even decide whether to appeal it, discourse kicks up that it’s for the best and that it was long past time to undo the transportation mask mandate. David Leonhardt writes a whole newsletter entry about how fun it was to fly unmasked. Leonhardt’s piece is filled with such trenchant observations as, “The trouble with the transportation mask mandate was that it was both too broad and too lenient.” He also couches the entire argument in what was by this point becoming a common refrain of his, that we can’t be sure that masking does anything, anyway, saying: “Rigorous laboratory tests show that masks reduce Covid transmission, but supporting real-world evidence tends to be much weaker.”
+
Also at the beginning of April, the Gridiron Dinner happens.
For those who don’t remember, this was a literal superspreader event attended by a bunch of Washington’s elite, including Fauci and Kamala Harris. It becomes a minor scandal.
It ended in at least 72 confirmed infections, which is a lot, considering that this number does not include infected staff who worked the event, since infections among staff were kept private and never disclosed.
Here are some highlights from the Washington Post’s account of the dinner:
[S]ome of the comic skits [at the event] featured actors dressed as the coronavirus, like large, green bouncing balls with red frills …
At one point, a performer dressed as Fauci sang from the stage to the real Fauci in the audience: “Doctor, doctor, give me some clues, we’ve got a bad case of covid blues.
+
13,000 people died of covid in April, according to the CDC
Again, 59% of them were vaccinated. 36% of them were boosted.
You may have noticed that there was much less activity on Covid from the Biden administration in April, apart from some dithering around the TSA mask mandate.
This will be characteristic of the rest of our timeline, beginning with Part III. There are long stretches in the remainder of 2022 where the Biden administration more or less seems to be trying to talk about covid as little as possible.
And in the background of this, we are becoming increasingly ill-informed about the state of the pandemic itself.
Programs are ending. Testing facilities are closing. People are being encouraged to use rapid tests at home, and none of those tests are being reported as positive test results by states, in part because there is no real mechanism to do so.
In other words, the Biden administration has by now successfully pivoted to a regime where cases don’t matter, only hospitalizations do. And as part of that pivot, the work they’ve done has also made it difficult to even understand how many cases are happening in most of the country
Recall the change to the Community Level system covered at the beginning of this section. The new Community Level system significantly increased the threshold of covid cases required to trigger a masking recommendation (importantly: recommendation, not mandate).
When you add to this decreased testing infrastructure, and substantially decreased, or increasingly infrequent, reporting by states of covid data, the bar is raised high for the CDC to ever broadly recommend masking again. Information on covid has dried up, and the processes the state used to employ to synthesize that information have also been subverted to paint a much rosier picture of covid risk in the US than the reality. It’s no surprise that, by May, the Washington Post asks: “How big is the latest U.S. coronavirus wave? No one really knows.”